More than 42 percent of American adults are now obese, according to the Centers for Disease Control and Prevention, and another 30 percent or so are overweight. Being overweight is defined as having a BMI (Body Mass Index) of 25-29, while those with a BMI of 30 or above are said to be obese.
“If you’re young and obese, you’re still at high risk despite your age,” says Justin Grodin, M.D., senior author of the study published today in Circulation. (In the study, young is defined as age 50 or younger.)
“In general, obese individuals are more likely to be hospitalized with COVID-19 than normal weight individuals,” adds Nicholas Hendren, M.D., a UTSW chief cardiology fellow and first author of the study, which will be presented this week at the American Heart Association Scientific Sessions 2020 conference. “In the hospital, obese individuals are at higher risk for death or the need for mechanical ventilation to help them breathe, even if they are young.”
The study’s findings should alert people who are overweight or obese – including those age 50 and under who may feel safe because of their age – that they are at greater risk from COVID-19, says Grodin, assistant professor of internal medicine at UT Southwestern. Those in the most severe category of obesity, called Class III and defined as having a BMI of 40 or higher, should be considered high risk and may warrant prioritization for a COVID-19 vaccine when it becomes available, Grodin adds. About 7 percent of the adult population falls into this category, according to the study.
While the numbers don’t explain why obesity worsens outcomes for COVID-19 patients, the study suggests several possibilities.
First, obesity is associated with diseases that have been linked to worse outcomes for COVID-19, such as hypertension and diabetes, according to the study. Secondly, the SARS-CoV-2 virus uses an enzyme called ACE2 to enter and infect human cells, and that enzyme is abundant in fat tissue. In addition, simply having more weight on the chest may make it harder for COVID-19 patients to breathe, Grodin says.
Also, negative effects tied to obesity may be especially apparent in younger patients because older COVID-19 patients have so many other risk factors, he adds.
The Circulation study analyzed data from more than 7,600 patients at 88 U.S. hospitals who were enrolled in the American Heart Association’s COVID-19 Cardiovascular Disease Registry. James de Lemos, M.D., a UTSW professor of internal medicine, helped create the registry along with volunteers and AHA staff. The Circulation study team adjusted its findings of risk to take into account patients’ age, sex, race, and prior health problems.
Looking at patients age 50 and under hospitalized for COVID-19, the researchers found that the vast majority – 85 percent – were either overweight or obese. That compares with 54 percent of patients over age 70, making weight more of a risk marker for the younger group. Among patients 50 and under, those with severe obesity had a 36 percent greater risk of dying, compared with normal weight individuals, the study found. Overall, adult patients with severe obesity had a 26 percent higher risk of dying.
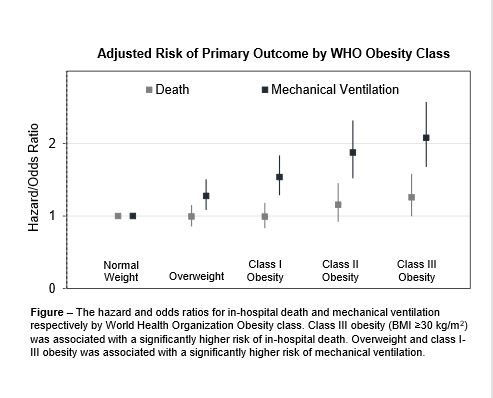
Looking at all adult patients, the risk of being sick enough to require a ventilator rose in lock-step as weight increased from overweight to Class III obesity, according to the study. The risk of death also rose for those who had Class III obesity.
“There is a greater proportion of obese people among those hospitalized for COVID-19,” says Grodin, “and obese patients are at higher risk for complications.”
In addition to greater risk for death and the need for ventilation, higher BMI also was linked to the need for kidney dialysis and the development of blood clots in deep veins and the lungs, according to the study.
Other studies are underway to examine how various patient characteristics affect COVID-19 risk, using the AHA’s COVID Registry, Grodin says.
Other UTSW researchers who participated in the study were de Lemos, Colby Ayers, Sandeep R. Das, Anjali Rao, Spencer Carter, Anna Rosenblatt, Anita A. Hegde, and Mark H. Drazner. Collaborators included Jason Walchok of the American Heart Association, Wally Omar of Beth Israel Deaconess Medical Center, Rohan Khera of Yale School of Medicine and Yale-New Haven Hospital, and Ian J. Neeland of University Hospitals Harrington Heart and Vascular Institute and Case Western Reserve University School of Medicine.
De Lemos holds the Sweetheart Ball-Kern Wildenthal, M.D., Ph.D. Distinguished Chair in Cardiology.
Relevant financial disclosures from the authors are included in the manuscript.
About UT Southwestern Medical Center
UT Southwestern, one of the premier academic medical centers in the nation, integrates pioneering biomedical research with exceptional clinical care and education. The institution’s faculty has received six Nobel Prizes, and includes 23 members of the National Academy of Sciences, 17 members of the National Academy of Medicine, and 13 Howard Hughes Medical Institute Investigators. The full-time faculty of more than 2,500 is responsible for groundbreaking medical advances and is committed to translating science-driven research quickly to new clinical treatments. UT Southwestern physicians provide care in about 80 specialties to more than 105,000 hospitalized patients, nearly 370,000 emergency room cases, and oversee approximately 3 million outpatient visits a year.

