To study these tumors and test new therapies, researchers at University of California San Diego School of Medicine use mice that bear glioblastoma tumor samples donated by patients who underwent surgery. With this approach, they recently discovered that treatment with both a targeted cancer therapy and the multiple sclerosis (MS) drug teriflunomide halts glioblastoma stem cells, markedly shrinks tumors and improves mouse survival.
The study is published August 7, 2019 in Science Translational Medicine.
“We used to think we’d find a single magic bullet to treat everyone with glioblastoma,” said senior author Jeremy Rich, MD, professor of medicine at UC San Diego School of Medicine and director of neuro-oncology and director of the Brain Tumor Institute at UC San Diego Health. “But now we realize that we need to find out what drives each patient’s unique tumor, and tailor our treatments to each individual.”
In recent years, the desire to personalize cancer therapies has led to the development of several targeted cancer therapies. These drugs work by inhibiting specific molecules that cancer cells rely on for growth and survival. For that reason, targeted therapies can work better and cause fewer side effects compared to traditional therapies, such as chemotherapy and radiation. Yet targeted therapies haven’t been as successful as the scientific community had hoped. According to Rich, that’s because it’s usually not enough to inhibit just one molecule or pathway driving tumor formation or survival — cancer cells will find a way to compensate.
“As scientists, we are often looking at small snapshot of what a cancer stem cell is doing,” said Rich, who is also a faculty member in the Sanford Consortium for Regenerative Medicine and Sanford Stem Cell Clinical Center at UC San Diego Health. “As a clinician, I also try to look at the bigger picture. I’m not looking for just one or two drugs to help my patients, because I think it’s going to take a whole personalized cocktail of many different drugs to really get the cancer cells on the run.”
To continue replicating, glioblastoma stem cells need to keep making more DNA, and to do that they need to make pyrimidine, one of DNA’s building blocks. Mining tumor genomic data available for hundreds of glioblastoma patients in six different databases, Rich’s team noticed that higher scores on pyrimidine metabolism were associated with poorer patient survival.
“It’s a lot of hard work to be a cancer cell. They have to work all the time to find ways to pull together pathways to survive and grow,” said Rich. “Not that I have sympathy for them. But knowing this helps us know where they might have weak spots.”
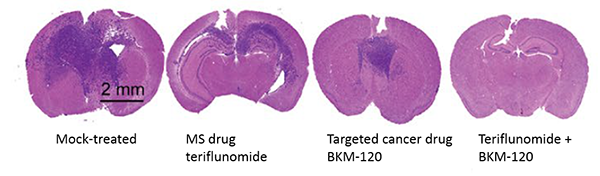
The MS drug teriflunomide happens to block pyrimidine-forming enzymes. Rich and team discovered that teriflunomide inhibits glioblastoma cell survival, self-renewal and tumor initiation in the laboratory. What’s more, the researchers found that when treated with teriflunomide alone, the patient-derived tumors shrank slightly and the mice bearing them survived somewhat longer, compared to mock-treated mice.
The team also tested two targeted cancer therapies: BKM-120, an inhibitor that works best in glioblastoma cells driven by lack of an enzyme called PTEN, and lapatinib, an inhibitor used to treat cancers driven by mutations in the Epidermal Growth Factor Receptor (EGFR). With BKM-120 treatment alone, tumors shrank moderately and mice survived even longer, compared to either mock-treated mice or teriflunomide-treated mice.
But when treated with both teriflunomide and BKM-120, tumors shrank markedly on average and the mice survived significantly longer, compared to mock-treated mice or mice who received either treatment alone.
“We’re excited about these results, especially because we’re talking about a drug that’s already known to be safe in humans,” Rich said. “But this laboratory model isn’t perfect — yes it uses human patient samples, yet it still lacks the context a glioblastoma would have in the human body, such as interaction with the immune system, which we know plays an important role in determining tumor growth and survival. Before this drug could become available to patients with glioblastoma, human clinical trials would be necessary to support its safety and efficacy.”
Co-authors include: Xiuxing Wang, Qiulian Wu, Shruti Bhargava, Zhe Zhu, Li Jiang, Zhixin Qiu, Linjie Zhao, Guoxing Zhang, Xiqing Li, UC San Diego; Kailin Yang, Cleveland Clinic and Case Western Reserve University; Leo J.Y. Kim, Ryan C. Gimple, Briana C. Prager, UC San Diego and Case Western Reserve University; Andrew R. Morton, Case Western Reserve University; Yu Shi, Ministry of Education of China; Wenchao Zhou, Weiwei Tao, Shideng Bao, Cleveland Clinic Lerner Research Institute; Sameer Agnihotri, Children’s Hospital of Pittsburgh and University of Pittsburgh; Paul S. Mischel, Ludwig Institute for Cancer Research, UC San Diego; and Stephen C. Mack, Baylor College of Medicine.
This research was funded, in part, by the National Institutes of Health (grants CA197718, CA154130, CA169117, CA171652, NS087913, NS089272, CA184090, NS091080, NS099175, NS073831).
###
Disclosure: Paul S. Mischel is a cofounder of Pretzel Therapeutics Inc., for which he owns equity and serves as a consultant.

