
The course of age-related macular degeneration (AMD), a leading cause of vision loss, is different in different people depending on the disease type. The wet form tends to progress faster than the dry form. Yet regardless of the type, for most people the decline in vision unfolds gradually over five years or more. Early AMD often affects only night vision; intermediate AMD affects daylight vision as well; late AMD impairs the ability to read or recognize familiar faces.
But for 10% to 20% of patients, AMD’s rate of progression and vision loss has an entirely different pace, going from diagnosis to late-stage AMD and legally blind in under five years.
Identifying who falls into this high-risk group often isn’t easy.
“Ascertaining a patient’s prognosis using the most widely available retinal imaging, called color fundus photography, requires significant clinical expertise,” said Emily Chew, M.D., director of the Division of Epidemiology and Clinical Applications at the National Eye Institute (NEI), part of the National Institutes of Health.
At the same time, specialists with the expertise to interpret retinal images for prognostic information are in short supply. Only a few thousand retinal specialists practice in the U.S. [1]
Even among expert readers there can be significant variability in how retinal images are interpreted. That’s because in many cases, patients fall along a spectrum where it’s difficult to categorize the risk.
“Discerning which AMD patients would benefit from an early, pull-out-all-the-stops approach can be a tough call,” said R. Theodore Smith, M.D., Ph.D., a retinal specialist at the New York Eye and Ear Infirmary of Mount Sinai. At the same time, patients and physicians need to know when urgent steps are needed to slow disease progression.
From the patient’s perspective, knowledge of one’s elevated risk for rapid vision loss may be an empowering motivator to make beneficial lifestyle changes. Smoking cessation and eating a diet rich in omega-3s from fish, such as salmon, and leafy greens can help slow disease progression.
Intraocular injections of anti-vascular endothelial growth factor (anti-VEGF) therapy can help maintain vision among patients with the wet form of AMD, but patients need to reach a threshold before the benefits outweigh the potential risks.
Such eye injections also are costly. For treating wet AMD, the U.S. Food and Drug Administration (FDA) has approved aflibercept (Eylea) and ranibizumab (Lucentis), which each cost around $2000 per injection. The two drugs are covered under Medicare Part B, but patients must meet their deductible first, and then pay 20% of the cost of the injections.
Anti-VEGF therapy slows the course of wet AMD by inhibiting the growth of new blood vessels. “It’s possible that a therapy that inhibits the growth of new blood vessels may have unintended effects on the cardiovascular system,” Smith said.
And evidence suggests it’s possible that anti-VEGF therapy (for wet AMD) contributes to the progression of dry AMD, which can co-occur in the same patient. So, starting anti-VEGF therapy, and determining how frequently to administer injections, involves a calculation of risk.
Emerging role for AI to predict late AMD
Researchers supported by the NEI are developing artificial intelligence/machine learning (AI/ML)-based systems that not only screen for AMD but also predict which patients will likely progress to late within two years. The systems also evaluate separately one’s risk for developing late wet (neovascular) AMD from one’s risk for late dry (geographic atrophy) AMD.
“This is important since treatment approaches for the two subtypes of late AMD are very different: Neovascular AMD needs prompt diagnosis, since delay in access to anti-VEGF therapy is usually associated with a poor outcome,” Chew said.
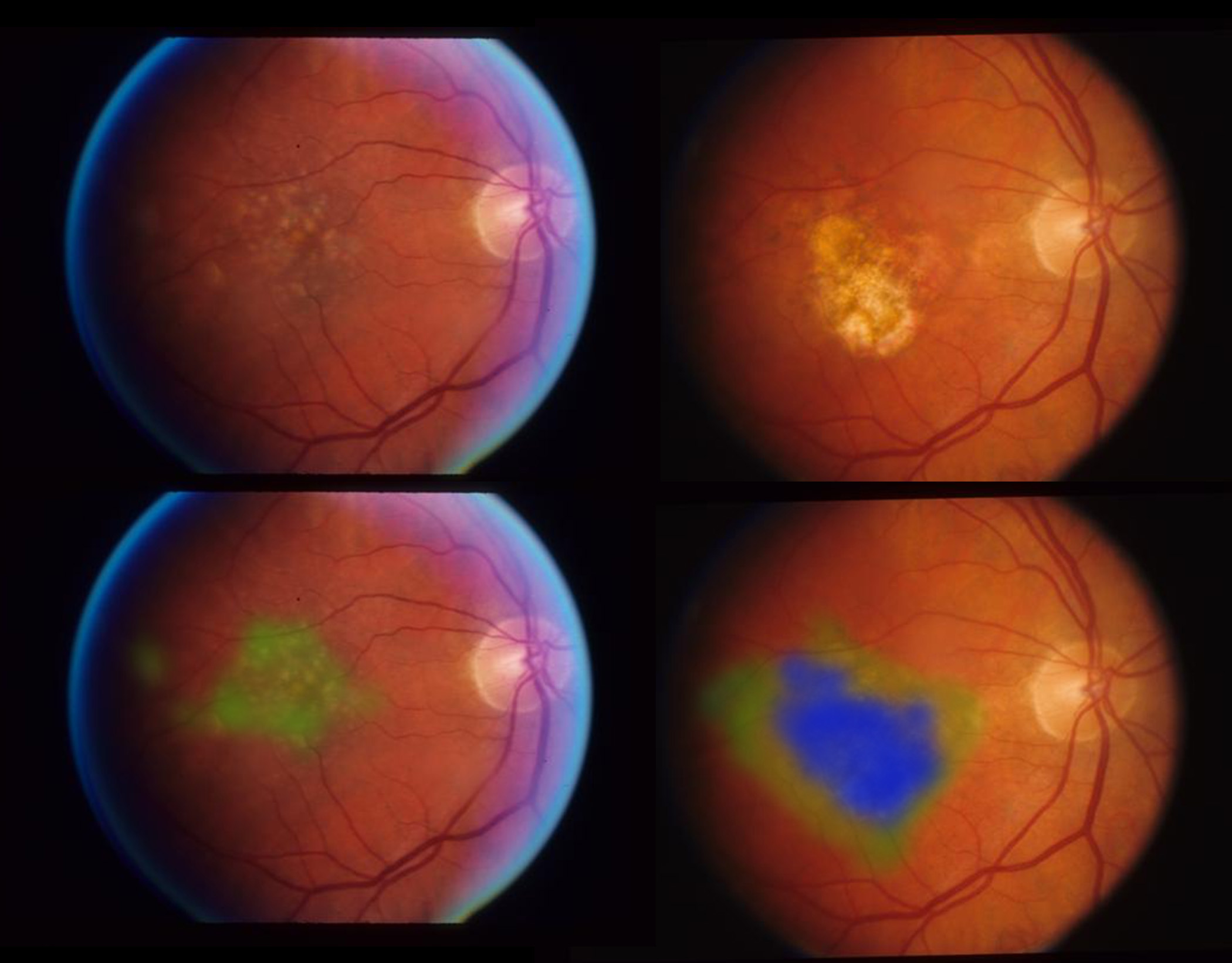
Such systems are autonomous, meaning that they can deliver clinical and diagnostic information on their own, without the need for expert interpretation. They are developed by training a deep convolutional neural network, a type of AI, on large datasets comprising thousands of patients with known outcomes. The network extracts features from these patients’ retinal images—features such as the size and type of drusen (small yellow deposits made up of fats and proteins) and pigment abnormalities. Imaging data are then combined with other patient data such as age, smoking status, genetic profile, and eye disease outcome. With enough data, the network begins to detect patterns that can aid screening and prediction.
iHealthScreen
iHealthScreen, located in Richmond Hill, New York, is an AI/ML-based system developer. Their iPredict enables non-eye care specialists to screen patients for AMD and to predict which individuals with early AMD are at risk for accelerated disease and vision loss.
Since 2015, iHealthScreen founder and chief scientist Alauddin Bhuiyan, Ph.D., has received more than $2 million from the NEI’s Small Business Innovative Research program, which funds independently owned companies with 500 or fewer employees to bring biomedical technologies to market.
Bhuiyan trained iPredict using 93,380 color fundus photos from the landmark NEI-funded Age-related Eye Disease Study (AREDS), led by Chew. The largest clinical trial of its kind, AREDS enrolled 4,757 participants, ages 55-80 years, and had cataract, AMD, or both. Patients were monitored for 10 years. Among the AREDS participants, 36 patients with early AMD converted to late AMD within one year, and 50 more within two years. Bhuiyan used 1824 images from individuals in these two groups (1824 images) and 2840 images from patients who did not convert, to train his prediction model.
The resulting model was then validated and tested using an additional 23,495 images from AREDS.
External validation relied on images collected for the Nutritional AMD Treatment-2 (NAT-2) study, which involved 263 patients who already had late AMD in one eye, and who were being monitored for the progression from early to late AMD in the other eye.
To use the iPredict system, a primary care provider takes color images of a patient’s retinas using a fully automated fundus camera. The fundus images along with other parameters (e.g., age, gender, smoking, etc.) are then securely transmitted to a centralized server where the iPredict AI/ML-based algorithm analyzes them for indications of AMD and its prognosis.
Within less than a minute, iPredict generates a report classifying the patient as referable or non-referable for AMD, along with recommendations to visit an ophthalmologist as necessary. Among those found to be referable, the system also generates a prediction score (on a 0 to 100% scale) quantifying the individual’s risk for developing late AMD within one year or two years.
In the AREDS dataset, iPredict predicted 2-year risk for progression to late AMD with 86% accuracy. For the NAT-2 dataset, that accuracy was 84%.[2]
The accuracy of the iPredict system in a non-specialist setting is being evaluated at four primary care clinics in the New York City area. For the study, primary care providers are using iPredict to screen 1000 adults, ages 50 and older, during their annual check-up. Results will be compared with assessments by retinal specialist.
“The greatest public health benefit is going to be screening in primary care clinics,” said Smith, who is the principal investigator for the study.
“iPredict’s screening model has been prospectively validated and has been submitted to the FDA. We are hopeful that we will have clearance to market the system to primary care practices by the end of 2023, and the prediction model will be aimed to be FDA-cleared in the future,” Bhuiyan said.
NIH developed AI-based late AMD prediction
A second AI/ML-based system for predicting late AMD was developed by NEI researchers, including Chew, in collaboration with colleagues from NIH’s National Center for Biotechnology Information.[3]
Like iHealthScreen, the NIH system was developed and validated using images from AREDS participants. However, it was trained and externally validated on an expanded set of images from participants who had intermediate AMD in both eyes when they enrolled in AREDS2, a separate clinical trial from AREDS.
The NIH model was trained to predict the probability of progression to late AMD based on 3298 participants (80,000 images) from both AREDS and AREDS2. When validated against an independent test dataset of 601 participants, the model outperformed the prognostic accuracy of retinal specialists using two clinical standards.
“A strength of our model is that it’s based on color retina photos taken over a 12-year period, and includes many more cases of disease progression,” said Chew.
Both iHealthScreen and the NIH system are trained to look for reticular pseudodrusen, a type of lesion that causes the retina to have a spotted pattern in the macula. The composition and location of the reticular pseudodrusen differ from that of typical drusen and they can be challenging to detect. Some data suggest reticular pseudodrusen are associated with a higher than usual risk for progression to late disease, but more research is needed about their underlying biology and prognosis.
Financial support for iHealthScreen was provided by grant R44EY031202, provided by the NEI Small Business Innovative Research program. Funding for Chew’s late AMD predication model was provided by the NEI Intramural Research Program.
The clinicaltrial.gov identifier for the trial of iHealthScreen in a primary care setting is ClinicalTrials.gov Identifier: NCT04863391.
To learn more about AMD, visit https://www.nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/age-related-macular-degeneration. To learn more about AREDS/AREDS2, visit https://www.nei.nih.gov/research/clinical-trials/age-related-eye-disease-studies-aredsareds2.
References
1. Pandit, R.R., et al., Distribution and Practice Patterns of Retina Providers in the United States. Ophthalmology, 2020. 127(11): p. 1580-1581.
2. Bhuiyan, A., et al., Artificial Intelligence to Stratify Severity of Age-Related Macular Degeneration (AMD) and Predict Risk of Progression to Late AMD. Translational Vision Science & Technology, 2020. 9(2): p. 25-25.
3. Peng, Y., et al., Predicting risk of late age-related macular degeneration using deep learning. npj Digital Medicine, 2020. 3(1): p. 111.
##
The Small Business Innovation Research (SBIR) program is a competitive awards-based funding mechanism that supports U.S.-based small businesses engaged in research and development that has the potential for commercialization. The NEI SBIR program specifically provides funding to companies developing technologies and innovations relating to blinding eye diseases, visual disorders preservation of sight, and addressing the special health problems and requirements of individuals with impaired vision.
NEI leads the federal government’s efforts to eliminate vision loss and improve quality of life through vision research…driving innovation, fostering collaboration, expanding the vision workforce, and educating the public and key stakeholders. NEI supports basic and clinical science programs to develop sight-saving treatments and to broaden opportunities for people with vision impairment. For more information, visit https://www.nei.nih.gov.
About the National Institutes of Health (NIH): NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit https://www.nih.gov/.
NIH…Turning Discovery Into Health®

