

I have been convinced of the importance of prevention in addressing mental-health problems since the early 1970s, when I began my doctorate in clinical psychology. But only now is there sufficient evidence from clinical trials of the effectiveness of preventive interventions, using approaches derived from interpersonal and cognitive behavioural therapy, to justify deploying them. And only now are the tools available to make such interventions available to people worldwide.
Two recent reports underline this conclusion. In February, the US Preventive Services Task Force, an independent panel of experts in evidence-based medicine, urged clinicians to “provide or refer pregnant and postpartum persons who are at increased risk of perinatal depression to counseling interventions”1. And last month, the US National Academies of Sciences, Engineering, and Medicine (NASEM) released a report2 calling on various stakeholders, from educators to policymakers, to prevent mental-health disorders and to promote healthy mental, emotional and behavioural development in the under 25s. (I was a member of the committees that prepared this document and two previous NASEM reports in 1994 and 2009 on preventive interventions3,4.)
The latest NASEM call to action2 is so all-encompassing, it is hard to know where to begin. I propose that initial efforts focus on preventing depression in pregnant women or in women who have recently given birth (perinatal depression). There is substantial evidence for the effectiveness of providing such women with basic skills in mood management5. These interventions could have an impact across generations, because better maternal mental health is linked to babies’ healthier development2. And if researchers and health-care systems were to monitor and compare the epidemiology of depression in thousands of mothers and their children in areas that have or have not deployed preventive interventions, stakeholders could measure their effect on entire communities.
Ultimately, massive open online interventions will need to be created (similar to the massive open online courses that are delivered on the Internet for free). These would allow anyone to obtain information and tools to help them stave off depression, at times and places that are convenient to them.
A global challenge
In the United States, nearly 15% of men and around 26% of women experience a major depressive episode at some point6. People are diagnosed with this if they report experiencing five of nine symptoms over at least two weeks. These must include either feeling depressed or being unable to feel interest or pleasure, as well as problems sleeping, changes in appetite, fatigue or having suicidal thoughts.
Numerous psychological, pharmacological and physical treatments are effective, such as cognitive behavioural therapy, antidepressant drugs and electroconvulsive therapy. But many people who are depressed are not receiving treatment7 because they fear stigma, can’t get to clinics or afford treatment, or because there aren’t enough psychologists and psychiatrists to meet their needs.
Given these challenges — and especially given the scale of the problem — societies worldwide need to take steps to stop depression from taking hold in the first place.
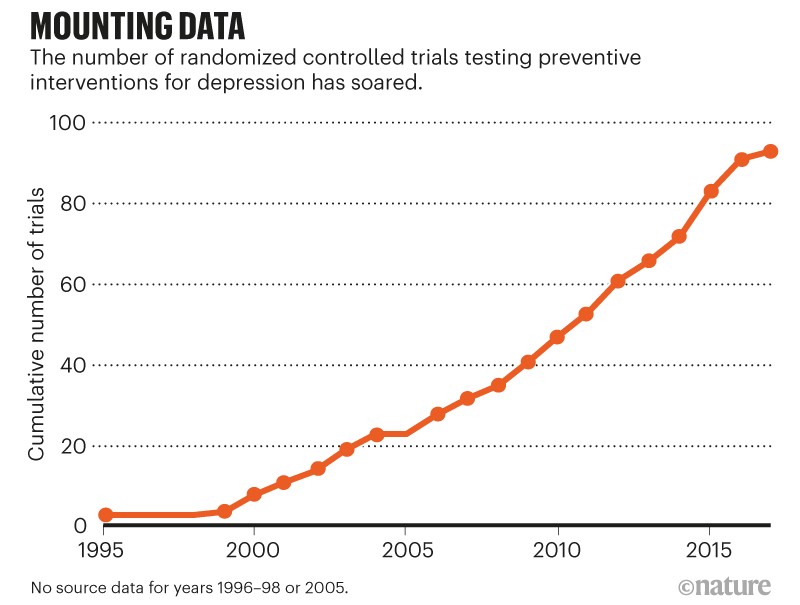
The number of randomized controlled trials testing preventive interventions has greatly increased since 1995 (see ‘Mounting data’). Two approaches have been studied the most: cognitive behavioural therapy and interpersonal therapy. The first involves teaching people how to use the natural relationship between thoughts, behaviours and mood to increase those thoughts and behaviours that lead to healthy mood states — and to reduce or modify those that elicit sadness, helplessness and hopelessness. (People might be asked, for instance, to predict how their mood would change if they undertook certain activities, such as seeing a friend — and then to record how their mood actually changed following the activity.) The second approach, interpersonal therapy, helps people to communicate better with others, and so to obtain more support from friends and family.

Sources: Refs 5, 9 & 10; https://go.nature.com/342TJWV
In the early 2000s in California, for example, my colleagues and I at San Francisco General Hospital (now the Zuckerberg San Francisco General Hospital and Trauma Center) conducted a pilot study funded by a US National Institute of Mental Health grant. The study involved 41 Spanish- and English-speaking women, most of whom were in their 16th week of pregnancy. These women were not clinically depressed but were deemed to be at high risk because they scored 16 or more on a depression scale, or had a history of major depressive episodes. The preventive intervention we used in this case involved psychologists teaching a cognitive behavioural ‘Mothers and Babies/Mamás y Bebés’ course in 2-hour sessions once a week for 12 weeks. Only 14% of the women taking the course had a depressive episode in the following year, compared to 25% in the control group8.
A meta-analysis of 32 studies in 2014 showed that, in all sorts of groups that are at risk — from expectant and new mothers to individuals who’d experienced a stroke — such preventive interventions reduce the onset of major depressive episodes by 21%, on average9. In the same year, my colleagues and I found that 15 of 42 randomized trials reported reductions of 50% or more in the incidence of depression10.
Then, this year, the US Preventive Services Task Force reviewed 50 randomized controlled trials testing preventive interventions specifically for perinatal depression. This has shown that, on average, such interventions reduce the incidence of major depressive episodes by 39%. However, one interpersonal approach, called ROSE, reduces the incidence of episodes by 50%, and the Mothers and Babies intervention reduces the incidence of episodes by 53%5.
In short, the data suggest that if we implement interventions that seem to be the most effective in clinical trials, we could halve the new cases of major depression.
So why focus on expectant or new mothers? I propose an initial focus on perinatal depression for four reasons. The evidence is strong. The window of risk is clear (during pregnancy and for a year after giving birth). Education and mood-management skills could be wrapped into the prenatal classes or home visits many pregnant women already receive, lowering cost and stigma — as was done in a 2010 study involving more than 2,000 women in the Trent area of England11. Most importantly, interventions could benefit multiple generations. A mother’s depression is associated with lower than average birthweight and preterm deliveries, as well as problems in children such as impaired cognitive development2. Conversely, the healthy development of babies and children could result in their having healthier, planned pregnancies when they themselves reach childbearing age.
Making it happen
Of course, rolling out evidence-based preventive interventions to millions of women at risk of perinatal depression all over a nation, or the world (many of whom don’t have access to prenatal or postnatal care), as well as to other high-risk groups such as adolescents, is a daunting proposition. The number of therapists or health workers available to provide cognitive behavioural courses or interventions based on interpersonal therapy is vastly inadequate, even when it comes to treatment. In 2013, for example, an estimated 43.8 million adults in the United States had experienced a mental illness in the past year, yet only 19.6 million received mental-health services. The World Health Organization estimates that, worldwide, more than 300 million people of all ages experience depression. Most do not receive treatment. A different strategy is required.
In 1998, with support from the Tobacco-Related Disease Research Program in Oakland, California, my colleagues and I began building an online resource to help people to quit smoking. We then conducted a randomized controlled trial in Spanish and English to determine whether people’s use of the site could generate quit rates comparable to those obtained from current smoking-cessation aids, such as the nicotine patch. (After six months, the quit rates of people using nicotine patches in the United States are 14–22%12,13.)
After registering on the site, people were able to access a guide on how to stop smoking. They could submit their ‘quit date’ and would then receive e-mails advising them on what steps to take as the date drew near. They were given instructions on how to manage their moods, and encouraged to keep diaries as part of the mood-management training. They also became part of an online community that offered support and information.
Our sample consisted of 1,000 smokers from 68 countries, 69% of whom provided follow-up data after one year. (If we didn’t get a response to our e-mails or phone calls, we assumed that person had resumed smoking.) In our study, 20% of Spanish speakers and 21% of English speakers quit14. In other words, we ‘matched the patch’.
Instead of shutting down the website at the end of the grant period, we continued to run the trial with a donation from the Brin Wojcicki Foundation in San Francisco. Over the following 6 years, data from more than 34,000 smokers from 168 countries generated similar results15,16. I realized then that our open online interventions were very similar to the now-popular massive open online courses. We had, in fact, carried out a proof-of-concept study of a massive open online intervention, or MOOI16.
Various online interventions have already helped to reduce symptoms of depression17. Australia’s moodgym programme, launched in 2001, is one of the oldest global online interventions for depression. With more than one million registered users, it could well be the most widely used computerized cognitive-behavioural programme in the world18. And this month, the UK National Health Service launched an online campaign called Every Mind Matters to help people maintain their mental health.
The interventions I’m calling for would be similar to these, but would need to be built such that their effectiveness could be evaluated on an ongoing basis. Also, effectiveness would need to be made transparent through continually updated ‘box scores’ on home pages; these could indicate, for instance, that the intervention resulted in a substantial improvement for 20% of 1,000 individuals. People would learn to look for the websites or apps that display effectiveness data, just as they look for services or films that have high ratings.
MOOIs (websites, apps, text-based interventions, and so on) could be provided at no charge to every expectant or new mother in the world — as well as to other groups at risk, such as adolescents, people who have lost a loved one or those who are experiencing physical-health problems. In communities where few people have access to the Internet, health clinics could provide resource rooms where people could access MOOIs. And in remote locations where there are no clinics, local providers could use tablets, laptops or mobile phones to share MOOIs with the people they serve. In fact, the Mothers and Babies course is already being implemented in Tanzania and Kenya.
Some might argue that large-scale implementation is premature if the risk of developing clinical depression can be cut by only 50%. But such rates of reduction are comparable to those for reducing the risk of influenza through vaccination (40–60%; see go.nature.com/2wjkr93).
Few online and smartphone apps for mental health have been rigorously tested. And some in the field might be concerned that MOOIs could be useless — or worse, harmful. All MOOIs would need to be evidence-based.
Another potential concern is that, once MOOIs become available, insurance companies could refuse to reimburse people for in-person sessions with counsellors. And there is the worry that MOOIs might exacerbate inequities, with wealthy people receiving cognitive behavioural therapy from therapists and poorer people having access only to online resources. But risks must be weighed against benefits for every intervention.
Thinking even bigger
So what about the other 50%, whose depression is harder to head off?
As all three NASEM reports2–4 point out, genetics, other biological factors — such as virus infections or hormone disorders — and people’s social and physical environments interact to have a major impact on mental health.
Epigenetics, the study of heritable alterations of the genome structure that are environmentally induced and don’t involve changes to the DNA sequence itself, is revealing how life events affect gene expression and the development of mental disorders. Much of the variation in DNA methylation that occurs during the first month of an infant’s life, as well as their weight at birth and even some childhood behaviours, have been associated with prenatal environmental factors, such as the mother’s smoking habits, mental health and body weight2.
The impact of the social environment on development has also been documented in detail. There is growing evidence that nurturing environments (achieved by rewarding good performance at school rather than punishing poor performance, for instance) have a major impact on children’s healthy development19.
To reach the other 50%, we need to expand beyond individually focused interventions. The 2019 NASEM report2 recommends that clinical researchers, health-care providers and policymakers should systematically study and implement more-ambitious interventions that focus on children’s social and physical environments.
Soon after arriving at the University of Oregon in Eugene in 1972 to start my doctorate in clinical psychology, I attended a talk at the local community mental-health centre. The speaker chided the professionals in the room, saying, in essence, “We therapists sit in our offices waiting for people to suffer enough to come to see us, or to be brought in by their family or the police because they are being disruptive. We should be going out into the community and sharing what we have learnt so that people can prevent the mental, emotional and behavioural problems that bring them to our offices.”
That evening, I decided to devote much of my professional work to the prevention of mental disorders.
Forty-seven years later, we have the knowledge and the tools to create a world in which fewer people ever experience clinical depression and other mental disorders. Let’s start creating it.

