
PHILADELPHIA – Genetically-edited immune cells can persist, thrive, and function months after a cancer patient receives them, according to new data published by researchers from the Abramson Cancer Center of the University of Pennsylvania. The team showed cells removed from patients and brought back into the lab setting were able to kill cancer months after their original manufacturing and infusion. Further analysis of these cells confirmed they were successfully edited in three specific ways, marking the first-ever sanctioned investigational use of multiple edits to the human genome. This is the first U.S. clinical trial to test the gene editing approach in humans, and the publication of this new data today in Science follows on the initial report last year that researchers were able to use CRISPR/Cas9 technology to successfully edit three cancer patients’ immune cells. Penn is conducting the ongoing study in cooperation with the Parker Institute for Cancer Immunotherapy and Tmunity Therapeutics.
“Our data from the first three patients enrolled in this clinical trial demonstrate two important things that, to our knowledge, no one has ever shown before. First, we can successfully perform multiple edits with precision during manufacturing, with the resulting cells surviving longer in the human body than any previously published data have shown. Second, thus far, these cells have shown a sustained ability to attack and kill tumors,” said Carl June, MD, the Richard W. Vague Professor in Immunotherapy and director of the Center for Cellular Immunotherapies in the Abramson Cancer Center and director of the Parker Institute for Cancer Immunotherapy at the Perelman School of Medicine at the University of Pennsylvania and the study’s senior author.
The findings are the latest milestone in Penn’s history as cellular and gene therapy pioneers, including development of the first FDA-approved CAR T cell therapy, Kymriah, for pediatric and adult blood cancer patients.
Patients on this trial were treated by Edward A. Stadtmauer, MD, section chief of Hematologic Malignancies at Penn, who is the co-lead author on the study along with Joseph A. Fraietta, PhD, an assistant professor of Microbiology at Penn. The co-senior author is Simon F. Lacey, PhD, director of the Translational and Correlative Studies Laboratory in the Center for Cellular Immunotherapies.
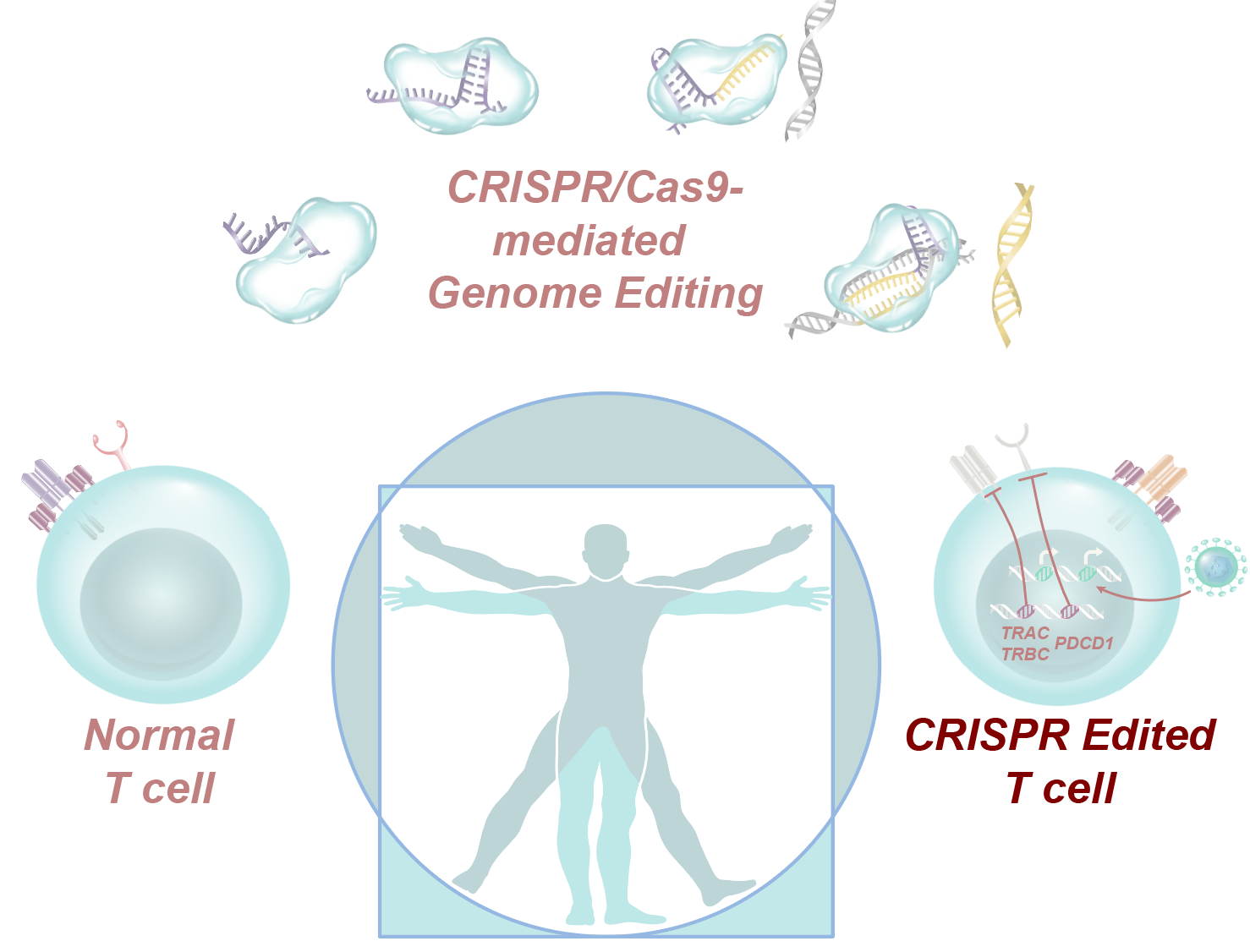
The approach in this study is closely related to CAR T cell therapy, in which patient immune cells are engineered to fight cancer, but it has some key differences. Just like CAR T, researchers in this study began by collecting a patient’s T cells from blood. However, instead of arming these cells with a receptor against a protein such as CD19, the team first used CRISPR/Cas9 editing to remove three genes. The first two edits removed a T cell’s natural receptors so they can be reprogrammed to express a synthetic T cell receptor, allowing these cells to seek out and destroy tumors. The third edit removed PD-1, a natural checkpoint that sometimes blocks T cells from doing their job.
“This new analysis of the three patients has confirmed that the manufactured cells contained all three edits, providing proof of concept for this approach. This is the first confirmation of the ability of CRISPR/Cas9 technology to target multiple genes at the same time in humans and illustrates the potential of this technology to treat many diseases that were previously not able to be treated or cured,” June said.
Once the three genes are knocked out, a fourth genetic modification was accomplished using a lentivirus to insert the cancer-specific synthetic T cell receptor, which tells the edited T cells to target an antigen called NY-ESO-1. Previously published data show these cells typically survive for less than a week, but this new analysis shows the edited cells used in this study persisted, with the longest follow up at nine months.
Several months after the infusion, researchers drew more blood and isolated the CRISPR-edited cells for study. When brought back into the lab setting, the cells were still able to kill tumors.
“Previous studies have shown these cells lose function within days, so the fact that the CRISPR-edited cells in this study retained anti-tumor function for a significantly longer period of time after a single infusion is very encouraging,” June said.
The CRISPR-edited T cells used in this study are not active on their own like CAR T cells. Instead, they require the cooperation of a molecule known as HLA-A*02:01, which is only expressed in a subset of patients. This means that patients had to be screened ahead of time to make sure they were a match for the approach. Participants who met the requirements received other clinically-indicated therapy as needed while they waited for their cells to be manufactured. Once that process was completed, all three patients received the gene-edited cells in a single infusion after a short course of chemotherapy. Analysis of blood samples revealed that all three participants had the CRISPR-edited T cells take root and thrive in the patients. While none responded to the therapy, there were no treatment-related serious adverse events.
CRISPR technology has not previously been tested in humans in the U.S. Investigators at Penn have pioneered a number of other “first uses” of engineered T cells over the past decade. Even with that experience, moving this work into the clinic while ensuring appropriate patient safeguards meant the research team had to move through a comprehensive and rigorous series of institutional and federal regulatory approval steps, including approval by the National Institutes of Health’s Recombinant DNA Research Advisory Committee and review by the U.S. Food and Drug Administration, as well as Penn’s institutional review board and institutional biosafety committee. The entire process required more than two years.
Researchers say these new data will open the door to later stage studies to investigate and extend this approach to a broader field beyond cancer, several of which are already planned at Penn.
This study was performed in cooperation with researchers from the Stanford University School of Medicine, including Kevin R. Parker, Yanyan Qi, Ansuman T. Satpathy, and Howard Y. Chang.
Additional Penn authors include Megan M. Davis, Adam D. Cohen, Kristy L. Weber, Eric Lancaster, Patricia A. Mangan, Irina Kulikovskaya, Minnal Gupta, Fang Chen, Lifeng Tian, Vanessa E. Gonzalez, Jun Xu, In-young Jung, J. Joseph Melenhorst, Gabriela Plesa, Joanne Shea, Tina Matlawski, Amanda Cervini, Avery L. Gaymon, Stephanie Desjardins, Anne Lamontagne, January Salas-Mckee, Andrew Fesnak, Donald L. Siegel, Bruce L. Levine, Julie K. Jadlowsky, Regina M. Young, Anne Chew, Wei-Ting Hwang, Elizabeth O. Hexner, Beatriz M. Carreno, Christopher L. Nobles, Frederic D. Bushman, and Yangbing Zhao.
The study was supported by the Parker Institute for Cancer Immunotherapy and Tmunity Therapeutics.
Editor’s note: Drs. June, Levine and Zhao are equity holders in Tmunity. Penn receives sponsored research funding from Tmunity, and as inventors of some of the licensed technology, Drs. June and Zhao, along with Penn, may receive additional financial benefits under the license in the future. Penn is also an investor in the company and holds equity interests.
###
Penn Medicine is one of the world’s leading academic medical centers, dedicated to the related missions of medical education, biomedical research, and excellence in patient care. Penn Medicine consists of the Raymond and Ruth Perelman School of Medicine at the University of Pennsylvania (founded in 1765 as the nation’s first medical school) and the University of Pennsylvania Health System, which together form a $7.8 billion enterprise.
The Perelman School of Medicine has been ranked among the top medical schools in the United States for more than 20 years, according to U.S. News & World Report’s survey of research-oriented medical schools. The School is consistently among the nation’s top recipients of funding from the National Institutes of Health, with $425 million awarded in the 2018 fiscal year.
The University of Pennsylvania Health System’s patient care facilities include: the Hospital of the University of Pennsylvania and Penn Presbyterian Medical Center—which are recognized as one of the nation’s top “Honor Roll” hospitals by U.S. News & World Report—Chester County Hospital; Lancaster General Health; Penn Medicine Princeton Health; and Pennsylvania Hospital, the nation’s first hospital, founded in 1751. Additional facilities and enterprises include Good Shepherd Penn Partners, Penn Home Care and Hospice Services, Lancaster Behavioral Health Hospital, and Princeton House Behavioral Health, among others.
Penn Medicine is powered by a talented and dedicated workforce of more than 40,000 people. The organization also has alliances with top community health systems across both Southeastern Pennsylvania and Southern New Jersey, creating more options for patients no matter where they live.
Penn Medicine is committed to improving lives and health through a variety of community-based programs and activities. In fiscal year 2018, Penn Medicine provided more than $525 million to benefit our community.
Original post https://alertarticles.info

