Untreated depression is associated with lower quality of life, poor treatment adherence, higher health care utilization and a risk for suicide up to 30 times higher than average.
Yet in most people with epilepsy, depression goes undetected. As an example, a Texas study conducted depression screening on 192 consecutive people visiting a high-volume epilepsy clinic. More than 1 in 4 people—26%—screened positive for depression and were subsequently diagnosed with depression. Of them, 65% had no previous history of the condition.
At the 33rd International Epilepsy Congress in Bangkok in June 2019, several sessions focused on psychiatric comorbidities in people with epilepsy and the crucial role of epileptologists in their identification and management.
“Sometimes we think too much about the epileptology and not enough about comorbidities,” said Mike Kerr (UK), co-chair of a session on neuropsychiatric issues in epilepsy. “There is individual clinician variation in this area. We must each recognize our own competency and know what we don’t know. Those are strongly influenced by our training, coworkers, culture, country and interests. But in the end, all clinicians must meet a minimum standard.”
This minimum standard was established by ILAE as part of its new epileptology curriculum. Domain 6 includes competencies and learning objectives about comorbidities, including the following:
6.1.1 Recognize psychiatric comorbidities, such as depression, anxiety, ADHD, psychosis and autism spectrum disorder
6.1.2 Appropriately manage or advise regarding psychiatric comorbidities
6.1.3 Adjust anti-seizure treatment as required by psychiatric comorbidities
However, the gap between knowledge and practice remains relatively wide. In a Bangkok session on psychological and psychiatric learning objectives in the ILAE curriculum, an informal survey found that most audience members did not conduct depression or suicidality screening in their clinics.
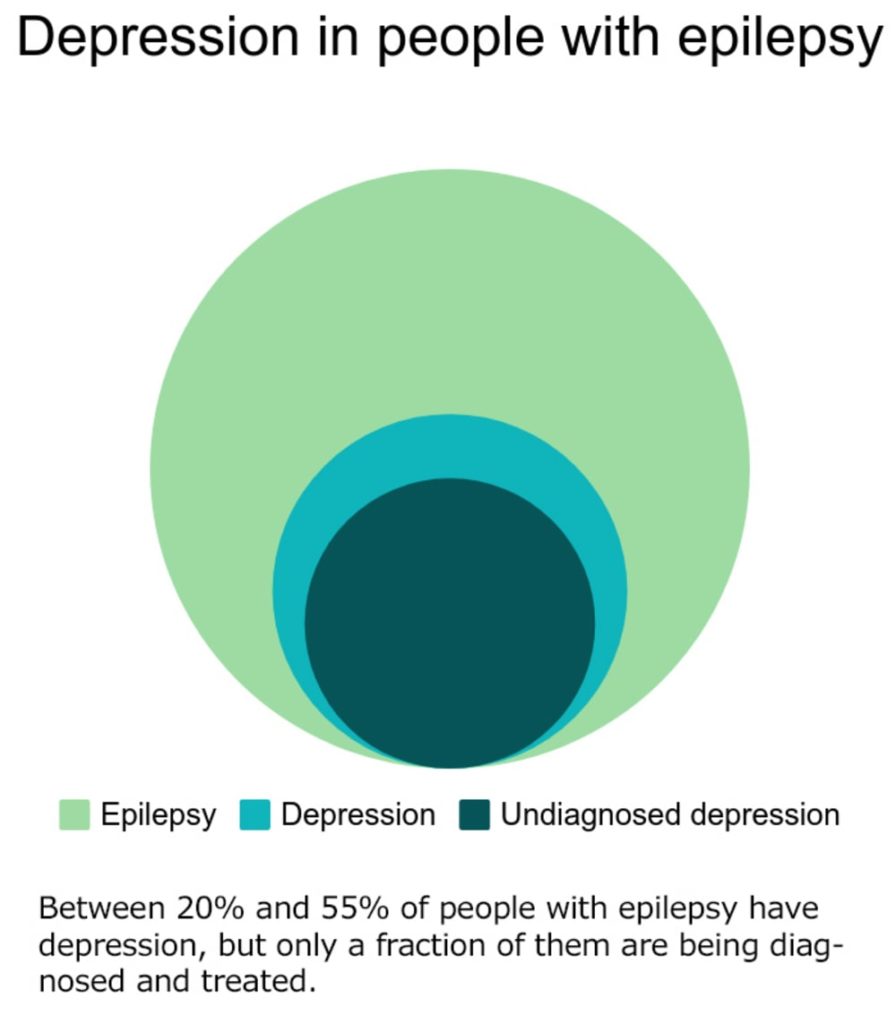
“Up to half of your patients will have depression and up to half will have anxiety,” said W. Curt LaFrance, Jr. (USA). “But almost no one in this session is using a depression screening tool.”
Generally, neurologists cite several reasons for not using screening tools or asking their patients about depression, including time constraints and the perception that screening is not their role. But physicians who manage the care of people with epilepsy are uniquely positioned to identify depression and initiate treatment that can improve quality of life and seizure control.
“It is part of our clinical responsibility as neurologists and epileptologists to take action in response to the high depression rates in people with epilepsy,” said Rosa Michaelis (Germany), co-chair of one of the sessions. “We should not expect other physicians to take over this task.”
Depression assessment: Individual variation
There’s no single “right” way for epileptologists to handle depression assessment and management, said Kerr. “Some people are multitaskers and will take on psychiatric management,” he said. “At the other end will be people who feel that none of it is their job. In the middle are the guiders, who keep epilepsy as a focus but also address the psychiatric issues.
Michaelis suggested that standardized screening is the most realistic strategy to increase detection rates. “We cannot rely on self-reported symptoms,” she said. Patients may not volunteer information about how they are feeling unless they are asked directly—and even then, they may deny or downplay their symptoms, or physicians may misinterpret their complaints. Screening tools provide valuable information in only a few minutes; they also can be a gateway to conversations about depression and suicidality.
If the idea of establishing a formal screening program is overwhelming, Kerr suggested being alert to the possibility of depression in every patient and merely asking one question: “During the last month, have you felt down, depressed, or hopeless, or had little interest or pleasure in doing things?”
If the answer sounds at all like “Yes,” refer the patient to a mental health professional. Alternatively, he said, “If you feel competent in mental health assessment, consider using a validated measure” to get a better idea of the extent and severity of the patient’s issue.
For screening, Kerr and others in Bangkok recommended the Neurological Disorders and Depression Inventory in Epilepsy (NDDI-E), which is free for public use and available in more than a dozen languages. The NDDI-E consists of six short “feeling” statements:
- Everything is a struggle
- Nothing I do is right
- Feel guilty
- I’d be better off dead
- Frustrated
- Difficulty finding pleasure
For each statement, the person indicates how often they felt that way over the past two weeks. Points are given for each answer: always or often (4 points); sometimes (3); rarely (2); never (1).
A cutoff of 15 points is generally used to suggest depression, though cutoffs of 11 to 16 have been reported. According to Kerr, a cutoff score of 15 has 81% sensitivity and 90% specificity.
The Patient Health Questionnaire-9 (PHQ-9) or a shorter form, the PHQ-2, also can be administered.
The ILAE Commission on Psychiatry recommends annual screening, but many of the experts urged more frequent screening. They noted that because depression can be episodic, more frequent screening will better identify those patients in need of treatment. It also may improve patient-physician communication and trust.
Though the ILAE consensus statement does not include a recommendation for anxiety screening, Kerr urged clinicians to screen for anxiety as well. The NDDI-E screens for both depression and anxiety; Kerr also recommended the GAD-2 or the ET7, short questionnaires that have been tested in people with epilepsy. Patients with positive screens can be referred to a mental health specialist or assessed further.
“All clinicians should aim to identify depression and anxiety,” Kerr said. “To be a level-2 epileptologist by ILAE standards, you will have to know how to do this.”
Antidepressants: Myth and reality
Psychotherapy and medication are common treatments for depression. Though few studies have focused on the effectiveness of psychotherapy for depression specifically in people with epilepsy, dozens of trials and several meta-analyses support the use of cognitive behavioral therapy (CBT).
Some medical professionals may avoid prescribing antidepressants to people with epilepsy because they believe these drugs decrease the seizure threshold. There is little scientific basis for this, say experts.
A 2017 study followed adults with epilepsy six months before and after the initiation of antidepressant therapy with selective serotonin reuptake inhibitors (SSRIs) or serotonin-norephinephrine reuptake inhibitors (SNRIs). Though the study was relatively small (N=84), the findings showed that antidepressants did not increase seizure frequency. In fact, among patients having more than one seizure per month at baseline, 27.5% went on to have less than 1 per month, and 48% had at least a 50% reduction in frequency. Of the patients, 73% had a therapeutic response to the antidepressant; changes in seizure frequency were independent of therapeutic response.
Pediatric screening
Janelle Wagner (USA) and Avani Modi (USA) addressed the issue of screening for depression and anxiety in the pediatric epilepsy population as it relates to two learning objectives in the ILAE curriculum:
- 2.5.1 – Recognize when to refer patients for a higher level of care (as it relates to psychiatric comorbidities)
- 2.9.1 – Provide counseling specific to children with epilepsy and their parents, according to the epilepsy types
Children with epilepsy are at higher risk than other children for depression, anxiety and attention deficit disorder, said Kette Valente (Brazil). Among children with epilepsy, 1 in 4 has depression, 1 in 4 has anxiety, and between 15% and 27% consider committing suicide.
A 2015 ILAE survey found that 55% of pediatric neurologists screened for these comorbidities, compared with only 7% in 2005. However, 50% of clinicians did not feel comfortable with their knowledge of anxiety, and only 40% said that screening for and managing comorbidities were priorities.
Depressive symptoms in children can look different than in adults, said Modi. Low self-esteem, cognitive symptoms, and negative thinking are common. Irritability and disruptive behavior also may be concerns, she said. “What may be seen as a conduct problem is actually depression.”
Valente, Wagner, and Modi described multiple screening instruments that take between 10 and 30 minutes to complete. Valente noted, however, that the instruments are often completed by parents, who do not always reflect their child’s behavior accurately.
The NDDI-E-Y, the pediatric version of the NDDI-E, had a sensitivity of 79% and a specificity of 92% in a 2016 validation study. Like the NDDI-E, the youth version can alert providers to suicidal ideation and provide a platform to discuss it.
Valente suggested screening children at their first visit, and then at certain time points:
- Every 6 months
- When seizures worsen
- After medication changes
- After any type of complaint about mood or behavior, whether it comes from the child or a parent or teacher
“Screening is not perfect, but it must be done,” she said. “There is no reason not to do it.”
Suicidality – what to do?
Jakob Christensen (Denmark) warned congress attendees that suicide risk overall is increasing worldwide, and that people with epilepsy have triple the risk of a suicide attempt and at least double the risk of death by suicide, compared with the general population. People with psychiatric comorbidities, and those recently diagnosed with epilepsy, are at even greater risk.
A recent meta-analysis found a prevalence of suicidal ideation of 23.2% among people with epilepsy—more than 7 times the prevalence in the general population. The pooled event rate of completed suicide in the meta-analysis was 0.5%, more than 30 times higher than the global estimated suicide rate (0.016%).
Screening can reveal suicidal thoughts or plans; on the NDDI-E, this can be seen on item 4, “I’d be better off dead”. A score of 3 or 4 on this item has been shown to identify suicidality with 84% sensitivity and 91% specificity.
Christensen recommended asking every patient about suicidal thoughts. “It can be as simple as saying, ‘Do you ever feel like life isn’t worth living?’ he said. Asking the question will not increase the risk of suicidality, he said. “People who have these thoughts are actually quite happy to have you ask the question. They often don’t realize that suicidality can be associated with epilepsy.”
If NDDI-E results indicate suicidality, Milena Gandy (Australia) outlined next steps:
- Ask the patient if they’ve thought about harming themselves in the past week. If they say yes, ask for details. Ask if they’ve ever tried to kill themselves and if so, how and when.
- If you feel they may be in imminent danger of harming themselves, ask if they can guarantee their safety until you see them again.
- If they ask for immediate help or can’t guarantee their safety, you can call a suicide hotline for them, refer them to the emergency room (or escort them there yourself), or refer them to a crisis service.
- If they are not in immediate crisis, refer them for mental health support if they don’t already have it. If they do have it, talk with them about making an urgent appointment.
The clock is ticking
Screening and conversations do take time. And while all physicians are pressed for time, “We need to think creatively about how we can do what’s possible” with screening, said Markus Reuber (UK). For example, ensure that any patient information (brochures, videos, other handouts) includes mention of mood disorders and anxiety as common comorbidities.
Reuber also noted that some offices and centers have epilepsy nurses or community health advocates who can talk about mental health, and mental health services, with patients. Providers must find creative ways to make time for these issues, he said, as they are a crucial part of epilepsy treatment.
“We can draw on experiences from other health conditions,” said Modi. “In cancer care, chronic pain and heart disease, referring to a psychologist is common practice. Yet there are still some perceptions in neurological disorders that psychological care isn’t as important. But improving mental health can improve medical care.”
##
Founded in 1909, the International League Against Epilepsy (ILAE) is a global organization with more than 120 national chapters.
Through promoting research, education and training to improve the diagnosis, treatment and prevention of the disease, ILAE is working toward a world where no person’s life is limited by epilepsy.
To learn more, visit our website or find us on Facebook.
Our website is available in multiple languages, and we’re on Twitter in English, French, Japanese, Portuguese and Spanish.
Original post https://alertarticles.info

